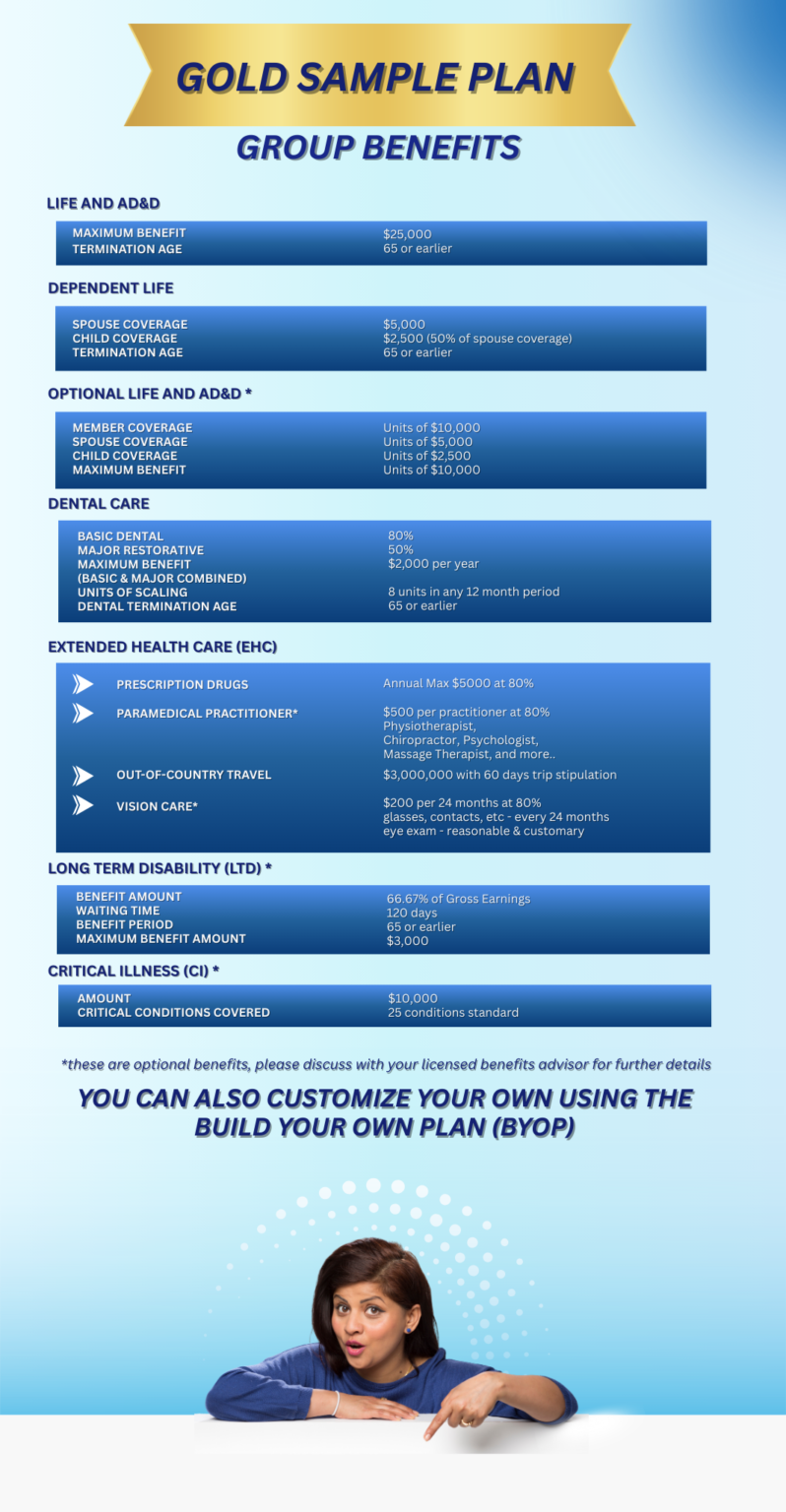
Sample Gold Plan
Here’s a sample gold plan, you can make changes if needed with higher or lower coverage by using our proprietary Build Your Own Plan (BYOP) template below. If you require assistance please BOOK A CONSULT or call 403-903-2898
Personalize Your Group Benefits Plan
If you’d like to customize your plan according to your preferences, please explore our “Build Your Own Plan” option.
BUILD YOUR OWN PLAN (BYOP)
{"field_096b6c1":{"display_mode":"show","fire_action":"All","file_types":"png","logic_data":[{"cfef_logic_field_id":"opt_maximum_benefit_fld","cfef_logic_field_is":"!=","cfef_logic_compare_value":"Other","_id":"58db17c"}]},"opt_maximum_benefit_other_fld":{"display_mode":"show","fire_action":"All","file_types":"png","logic_data":[{"cfef_logic_field_id":"opt_maximum_benefit_fld","cfef_logic_field_is":"==","cfef_logic_compare_value":"Other","_id":"58db17c"}]},"field_cc5f09c":{"display_mode":"show","fire_action":"All","file_types":"png","logic_data":[{"cfef_logic_field_id":"para_maxbenefit_fld","cfef_logic_field_is":"!=","cfef_logic_compare_value":"Other","_id":"42d90bc"}]},"field_6c00e90":{"display_mode":"show","fire_action":"All","file_types":"png","logic_data":[{"cfef_logic_field_id":"para_maxbenefit_fld","cfef_logic_field_is":"==","cfef_logic_compare_value":"Other","_id":"42d90bc"}]},"field_6e6c45b":{"display_mode":"show","fire_action":"All","file_types":"png","logic_data":[{"cfef_logic_field_id":"para_maxbenefit_fld","cfef_logic_field_is":"==","cfef_logic_compare_value":"Other","_id":"42d90bc"}]},"field_63ed082":{"display_mode":"show","fire_action":"All","file_types":"png","logic_data":[{"cfef_logic_field_id":"para_maxbenefit_fld","cfef_logic_field_is":"!=","cfef_logic_compare_value":"Other","_id":"42d90bc"}]},"field_e39592c":{"display_mode":"show","fire_action":"All","file_types":"png","logic_data":[{"cfef_logic_field_id":"vis_eye_exam_fld","cfef_logic_field_is":"==","cfef_logic_compare_value":"Adult: $x per 24 month child:$x per months","_id":"4c8ba51"}]},"field_cb6e8d0":{"display_mode":"show","fire_action":"All","file_types":"png","logic_data":[{"cfef_logic_field_id":"vis_eye_exam_fld","cfef_logic_field_is":"!=","cfef_logic_compare_value":"Adult: $x per 24 month child:$x per months","_id":"d76b95b"}]},"field_7c7fea8":{"display_mode":"show","fire_action":"All","file_types":"png","logic_data":[{"cfef_logic_field_id":"vis_glasses_fld","cfef_logic_field_is":"==","cfef_logic_compare_value":"Adult: $x per 24 month child:$x per months","_id":"78c0271"}]},"field_1349e83":{"display_mode":"show","fire_action":"All","file_types":"png","logic_data":[{"cfef_logic_field_id":"vis_glasses_fld","cfef_logic_field_is":"!=","cfef_logic_compare_value":"Adult: $x per 24 month child:$x per months","_id":"d76b95b"}]},"field_c06123c":{"display_mode":"show","fire_action":"All","file_types":"png","logic_data":[{"cfef_logic_field_id":"cri_critical_conditions_covered_fld","cfef_logic_field_is":"!=","cfef_logic_compare_value":"Other","_id":"adcd42f"}]},"field_cric_other":{"display_mode":"show","fire_action":"All","file_types":"png","logic_data":[{"cfef_logic_field_id":"cri_critical_conditions_covered_fld","cfef_logic_field_is":"==","cfef_logic_compare_value":"Other","_id":"adcd42f"}]},"field_xvalue":{"display_mode":"show","fire_action":"All","file_types":"png","logic_data":[{"cfef_logic_field_id":"long_benefit_amount_fld","cfef_logic_field_is":"==","cfef_logic_compare_value":"X% of the first $X of the monthly earnings","_id":"e4096bb"}]},"field_plusx":{"display_mode":"show","fire_action":"All","file_types":"png","logic_data":[{"cfef_logic_field_id":"long_benefit_amount_fld","cfef_logic_field_is":"==","cfef_logic_compare_value":"plus X% of the balance","_id":"e4096bb"}]},"field_9a31283":{"display_mode":"show","fire_action":"All","file_types":"png","logic_data":[{"cfef_logic_field_id":"long_benefit_amount_fld","cfef_logic_field_is":"!=","cfef_logic_compare_value":"X% of the first $X of the monthly earnings","_id":"e4096bb"}]}}